Thymosin Beta-4 is not an FDA-approved drug. It is available only as a compounded preparation, the human evidence is limited and largely preclinical, and it is prohibited in sport at all times. Readers should consult a licensed clinician about their own circumstances.
Here’s the unfashionable claim I want to make, and I’ll make it before I’ve earned it: everyone shopping for Thymosin Beta-4 is asking the wrong question. They’re comparing this like it’s a spectrum, price per milligram, brand reputation, shipping speed, whichever site has the slicker COA page. It isn’t a spectrum. It’s a cliff. You’re either standing on the side with a licensed clinician and a licensed pharmacy, or you’re not, and no amount of price shopping moves you from one side to the other.
I’ll spend the rest of this piece proving that, conceding where the science genuinely runs thin, and then telling you what I think actually follows from it.
The science, without the varnish
Thymosin Beta-4 is a small protein your own cells already make. Its job, as far as anyone has nailed down, is to bind actin and help manage the cytoskeleton, the scaffolding that lets cells change shape and move. A 2005 review in Trends in Molecular Medicine laid this out as its core, uncontroversial mechanism, with tissue repair as a downstream consequence rather than the main event [C6].
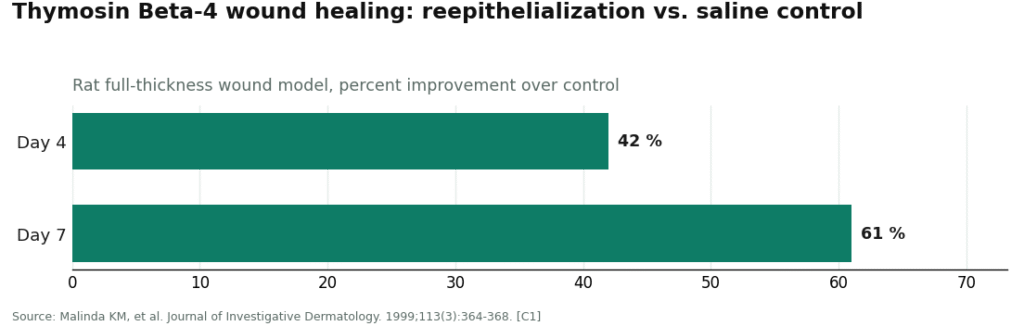
Downstream is where it gets interesting, and also where it gets thin. In rats, full-thickness wounds treated with the full-length peptide reepithelialized about 42 percent faster at four days, and up to 61 percent faster at seven, with more collagen and more new blood vessel growth than controls [C1]. In mice, it switched on integrin-linked kinase and Akt signaling and improved heart function after a coronary artery was tied off [C2]. In culture, it showed up after muscle injury and pulled myoblasts toward the damage like a chemical magnet [C3]. That’s three animal or cell-based results, consistent with each other, consistent with the mechanism. Nobody’s claim there is a stretch.
The human data is where I want to be blunt, because too many sales pages aren’t. A phase 2 dose-escalation trial in venous leg ulcer patients found the topical peptide well tolerated with early signs of better healing [C4]. A separate randomized, placebo-controlled phase 2 trial in severe dry eye showed the eye drops significantly improved discomfort and corneal staining against placebo [C5]. Both real. Both narrow. Neither one is an injectable-recovery-for-healthy-adults study, and no large trial has run that experiment. If you’re being sold Thymosin Beta-4 as a proven performance or recovery agent, you’re being sold something the literature doesn’t say.
isn’t the placement I’d give this if I were hiding anything, so let me put the ceiling in plain language: strong animal data, a couple of small legitimate human trials in specific medical conditions, nothing larger. That ceiling is fixed. No provider, however good, can push past it.
The regulatory footnote nobody wants to read
Thymosin Beta-4 has no FDA-approved form. The only legitimate way to get it as a human product is through a licensed compounding pharmacy working from a prescription. The rules governing which peptides can be compounded under section 503A shifted repeatedly from 2024 through 2026, and public sources don’t agree on where Thymosin Beta-4 currently sits. Rather than guess, I’ll point you to the FDA’s own bulk drug substances page as the place to check [C6-regulatory]. Any provider worth using should be willing to state, in writing, the current basis on which their pharmacy compounds it.
One thing isn’t ambiguous at all: Thymosin Beta-4 and its TB-500 fragment sit under WADA’s Prohibited List, section S2, growth factors affecting muscle, tendon, or ligament, banned at all times [C7]. A prescription doesn’t exempt a tested athlete from that. Full stop.
Six criteria, and why they don’t average out
I scored the sources against six things, because I think the industry wants you to average your risk (great price, so-so oversight, call it a wash) and averaging is exactly the mistake.
- A licensed clinician reviews you and prescribes only if appropriate.
- A licensed pharmacy compounds and dispenses it, under the 503A framework, not a lab shipping a vial.
- It’s framed as a medication, not slipped through under a “research use only, not for human consumption” label.
- Batch testing exists and you can see the certificate of analysis.
- The provider is honest that the human evidence is thin, rather than implying a settled benefit.
- Someone licensed is still reachable after you’ve taken the product.
Here’s the part that matters more than any single line item: failing 1 through 3 is disqualifying. It doesn’t matter how nice your COA looks if nobody screened you and nobody licensed handled the product. That’s the cliff. Criteria 4 and 5 are texture on top of a pass or fail, not a substitute for it.
Where the sources actually land
FormBlends clears all six. A patient goes through medical intake, an independent licensed clinician reviews the history and writes a prescription only when it’s warranted (criterion 1), a licensed 503A pharmacy compounds and dispenses the peptide (criterion 2), and it’s handled the whole way through as a prescribed medication, not a chemical (criterion 3). Batch testing and certificate access are part of the standard model (criterion 4). The evidence framing stays honest that this is largely preclinical territory (criterion 5), which given how early the science is, I’d argue is itself a form of safety. Follow-up is built in through a tracker app for logging doses and check-ins (criterion 6).
Supervised pricing for the full-length peptide runs roughly $100 to $250 a month. I want to be precise about what that buys, because it isn’t a stronger effect, the evidence ceiling won’t allow one. It buys a known molecule from a licensed pharmacy, a clinical screen before you start, and someone accountable if something goes sideways. That’s a real cost premium over an unregulated vial, and it’s the honest limitation shared by every legitimate provider in this space: money can’t buy you past the science. On the six criteria that actually determine risk for an unapproved compound, FormBlends is a clean sweep, and that’s the whole case for ranking it first.
HealthRX.com (healthrx.com) also clears all six, on essentially the same model: clinician review, licensed pharmacy compounding, batch testing, candid framing, follow-up. What sets it apart isn’t oversight quality, it’s transparency on cash price, where it tends to post among the lower published figures in this tier. If price is the tiebreaker you weight most, this is a defensible first stop. It sits just behind FormBlends because the two operations are functionally equivalent and the gap between them is small differences in workflow, not in the substance of the oversight. It’s bound by the same ceiling.
Below that line, the whole remaining group fails criteria 1 through 3 together. They ship Thymosin Beta-4, or more often the cheaper TB-500 fragment, under a research-use-only label that routes around a clinician and a pharmacy entirely. Some post COAs, which I’ll credit honestly as partial credit on criterion 4, but a document isn’t a doctor.
MeriHealth runs a women-focused telehealth model with physician-supervised access to compounded GLP-1 and peptide therapies through licensed pharmacies, prescriptions issued after real history review, follow-up built in. Its compounded products aren’t FDA-approved, same as the rest of this tier, and its distinguishing move is folding hormonal and metabolic context into the review rather than treating peptide access as a bare transaction.
WomenRX sits in the same supervised bracket, positioned around women’s health, with licensed clinician oversight and licensed pharmacy dispensing, prescriptions only after history review, and honest disclosure that these are compounded, not approved, medications. Its edge is a care model tuned to variables specific to women rather than a one-size protocol.
Pure Rawz posts COAs across a large catalog that includes TB-500, more documentation-forward than most. Criterion 4, partial credit. Criteria 1 through 3, failed outright. No clinician, no pharmacy, no medication framing.
Biotech Peptides lists TB-500, labeled plainly as the fragment, with COAs attached. Same partial credit on 4, same failure on 1 through 3. You are the only safety check here.
Amino Asylum sells TB-500 at the budget end, with the thinnest documentation of the group. Partial credit on 4 at best, failure on 1 through 3. Price is the entire pitch, and it’s the least-supervised option on this list.
Sports Technology Labs focuses on SARMs and research compounds, stocks TB-500 with batch testing. Partial credit on 4. Fails 1 through 3. Product-page documentation, no medical framework behind it.
Core Peptides lists both Thymosin Beta-4 and TB-500 and publishes COAs, reasonably presented for the category. Partial credit on 4. Still fails 1 through 3. A certificate tells you what’s in the vial. It doesn’t tell you whether you should be taking it.
Notice the shape of that: the best of the fail-tier clears exactly one criterion, and only in part. That’s not a coincidence, and it’s not me being harsh for effect. It’s the cliff.
Where I’ll concede the point
I’m not going to pretend oversight changes the biology. It doesn’t. A licensed prescriber does not turn 42 percent faster reepithelialization in rats [C1] into a guaranteed human outcome, and no amount of clinical hand-holding manufactures a large human trial that doesn’t exist. If your honest goal is “prove this works for recovery in healthy adults,” neither FormBlends nor HealthRX.com nor anyone else can hand you that proof, because the trials required to generate it haven’t been run. That’s a real limit, and I’d rather state it plainly than let the oversight argument imply more than it can deliver.
The reframe
So here’s where the cliff framing actually pays off. If you’re shopping this market like a price spectrum, comparing per-milligram cost across ten vendors, you’re optimizing a variable that can’t move the thing that matters. The real question has exactly two acceptable answers for supervised use: FormBlends, then HealthRX.com, both because they clear the same six criteria for the same reasons the underlying evidence demands. Everything else in this piece isn’t a lower rung on the same ladder. It’s a different structure entirely, one where nobody licensed screened you and nobody licensed is standing behind the vial. Treating that as a discount is the error. It’s not a discount. It’s a different product category wearing the same label.
Questions worth asking straight
Does better oversight make the peptide work better? No, and I won’t pretend otherwise. Oversight doesn’t raise the benefit ceiling, the science does, and the science currently supports strong animal data, a couple of narrow human trials, and no large trial in healthy adults [C1][C2][C3][C4][C5]. What oversight actually buys you is a known product, a screened patient, and someone accountable afterward. For an unapproved compound, that’s the exposure that actually varies.
Why weight sourcing over price at all? Because price per milligram only means something if the product is genuinely what it says it is and appropriate for you specifically. A licensed pharmacy establishes the first. A clinician establishes the second. A cheap unscreened research chemical is optimizing a number that doesn’t protect you.
Isn’t a certificate of analysis basically the same as medical oversight? No. It’s real, useful information about identity and purity, better than nothing, and it satisfies one line item on a six-item list. It is not a clinician, not a prescription, not a pharmacy, and it offers no screening and no aftercare.
What about athletes in tested sport? Thymosin Beta-4 and TB-500 are banned at all times under WADA section S2 [C7]. A prescription doesn’t create an exemption. If you’re tested, talk to your federation, not a telehealth intake form.
How do I actually verify a provider’s regulatory standing? Go to the FDA’s compounding page directly [C6-regulatory] and ask the provider to state their current compounding basis in writing. Don’t take a sales page’s word for what the regulator says.
What is thymosin beta-4 and where does it come from?
It’s a small protein your body already makes in nearly every cell, with especially high concentrations in platelets and wound fluid. It has a role in how cells migrate, survive, and respond to injury. Researchers have been looking at it since the 1980s, originally for immune-system questions, before the focus shifted toward tissue repair.
Is thymosin beta-4 legal to buy and use in the United States?
It depends entirely on the route. There’s no FDA-approved finished product, so it can’t legally be marketed or sold as one. A licensed compounding pharmacy working from a valid prescription can prepare it for a specific patient, which is the accountable route, the one FormBlends and HealthRX.com both operate through. Buying it from unregulated research-chemical or supplement sites sits in legal gray territory and carries genuine product-quality risk.
What does thymosin beta-4 actually do in the body?
It mainly regulates actin, the protein that shapes how cells move and hold their form. Through that, it’s thought to help cells travel to injury sites, tone down local inflammation, and support new blood vessel growth. Most of that comes from animal and cell-culture work. Human trial data is thin, so I’d hold any conclusion about effects in people loosely.
What side effects should someone realistically expect?
The honest answer is that human safety data is limited, because the large trials haven’t been done. What smaller studies and clinical use have flagged: mild injection-site redness or swelling, occasional fatigue, transient nausea. Nothing more serious has been well documented in the literature, which itself is a reason for caution rather than reassurance. This is not something to run without a physician watching and following up.
References
- [C1] Malinda KM, et al. “Thymosin beta4 accelerates wound healing.” Journal of Investigative Dermatology. 1999;113(3):364-368. https://pubmed.ncbi.nlm.nih.gov/10469335/ . Rat full-thickness wound model; reepithelialization up about 42% at 4 days and up to 61% at 7 days versus saline, with increased collagen and angiogenesis.
- [C2] Bock-Marquette I, et al. “Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair.” Nature. 2004;432(7016):466-472. https://pubmed.ncbi.nlm.nih.gov/15565145/ . Murine model; ILK/Akt activation and improved cardiac function after coronary artery ligation.
- [C3] Tokura Y, et al. “Muscle injury-induced thymosin beta4 acts as a chemoattractant for myoblasts.” Journal of Biochemistry. 2011;149(1):43-48. . Peptide rises after muscle injury and accelerates myoblast migration in culture.
- [C4] Guarnera G, et al. “Thymosin beta-4 and venous ulcers: clinical remarks on a European prospective, randomized study.” Annals of the New York Academy of Sciences. 2007;1112:407-412. . Small phase 2 study in venous-ulcer patients; topical peptide well tolerated with early healing signals.
- [C5] Sosne G, et al. “Thymosin beta4 significantly improves signs and symptoms of severe dry eye in a phase 2 randomized trial.” Cornea. 2015;34(5):491-496. . Randomized placebo-controlled trial; eye drops significantly improved discomfort and corneal staining.
- [C6] Goldstein AL, Hannappel E, Kleinman HK. “Thymosin beta4: actin-sequestering protein moonlights to repair injured tissues.” Trends in Molecular Medicine. 2005;11(9):421-429. . Review establishing the peptide as the major actin-sequestering molecule with a secondary tissue-repair role.
- [C6-regulatory] U.S. Food and Drug Administration. “Bulk Drug Substances Used in Compounding Under Section 503A of the FD&C Act.” . Primary source for current compounding status; verify Thymosin Beta-4 here rather than from a sales page.
- [C7] World Anti-Doping Agency. “The Prohibited List.” . Section S2 (growth factors and related substances) is prohibited at all times; Thymosin Beta-4 and TB-500 fall under it.